India has no unified health record system. Patients carry paper folders to every appointment, lose prescriptions between visits, and have no way to track their own medical history over time. I designed Practo's personal health records from the ground up: a temporal data model, automated doctor-to-patient record sharing, and a patient-facing interface that made 56 million medical records accessible, organized, and useful.
The problem
Chronic patients (those managing diabetes, hypertension, arthritis) accumulate dozens of records across years of treatment. In India, these records live in physical folders, handed between doctors in manila envelopes. Prescriptions get lost. Lab results are forgotten. Patients arrive at appointments unable to recall what medication they're on or when they last had blood work done.
Practo had a basic file upload feature, but it wasn't solving the real problem. Ethnographic research, analytics review, and interviews with doctors confirmed: patients needed a system that understood their health journey, not a file cabinet in the cloud.
Research
I interviewed 40 patients managing chronic conditions and ran diary studies to understand how they stored, retrieved, and shared health records in their daily lives. The findings exposed how deeply broken the paper-based system was.
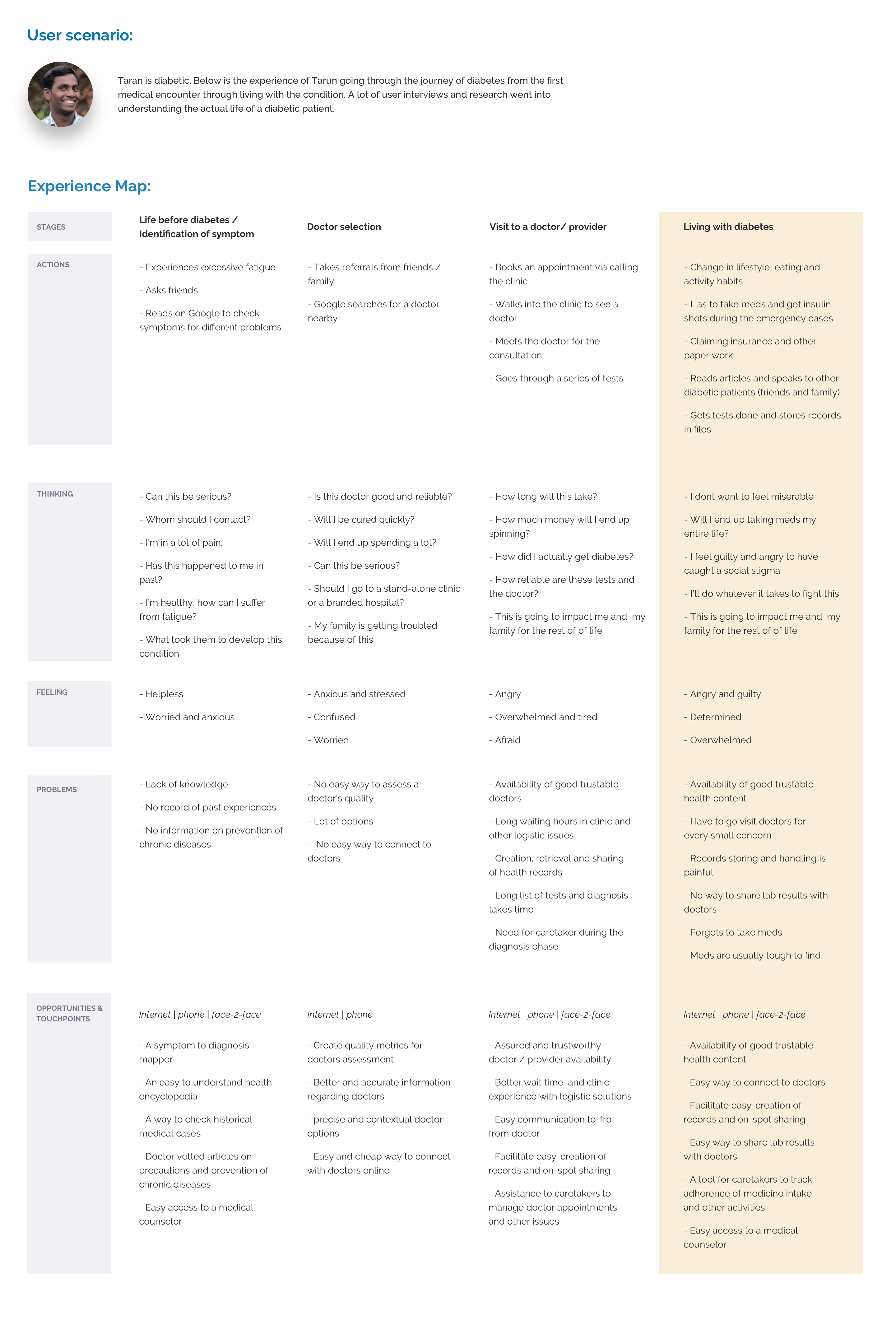
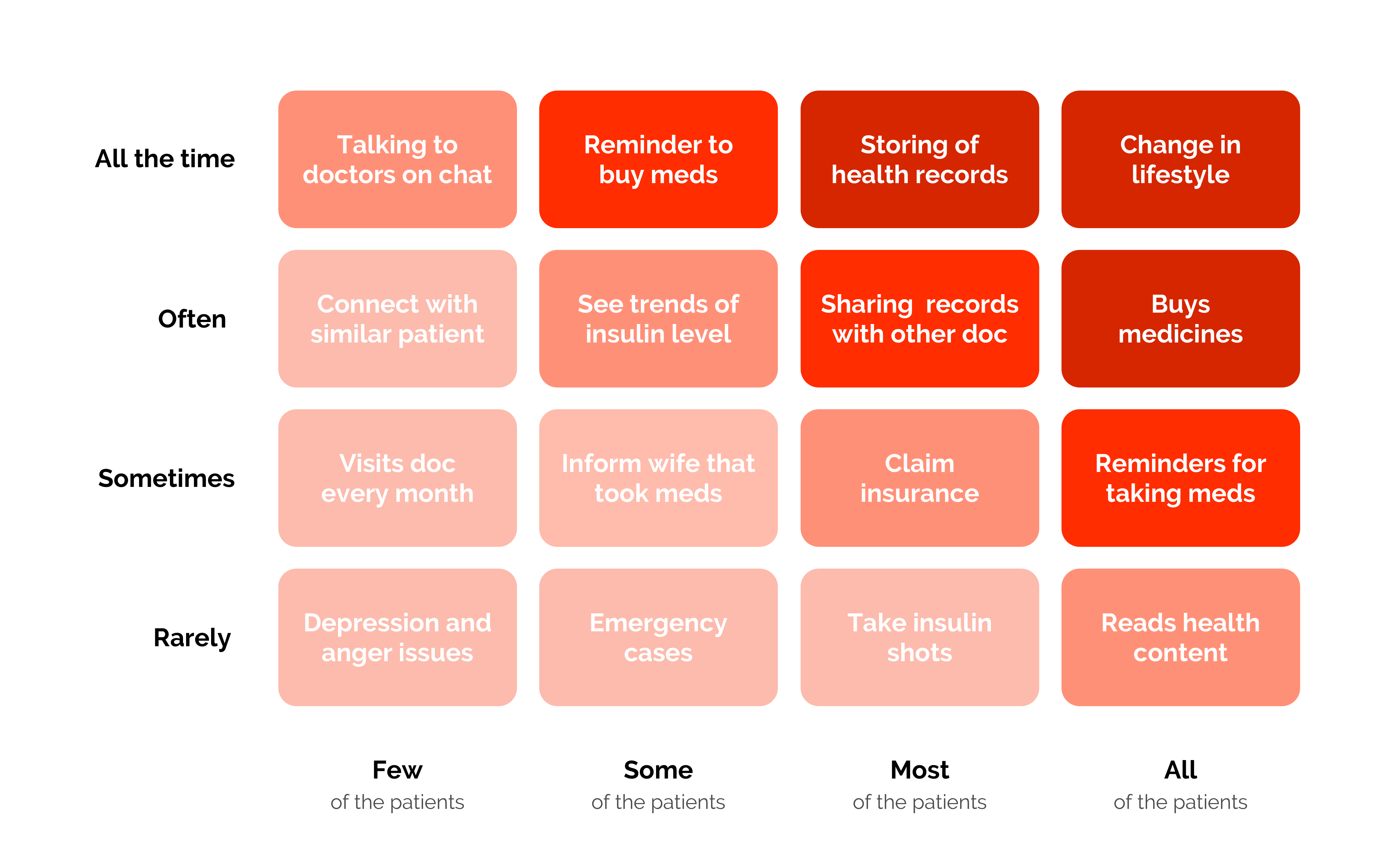
The broader Practo app addressed the first three stages of the patient journey: finding a doctor, booking, and consulting. PHR focused entirely on stage four: ongoing health management after the consultation ends. A Red Routes analysis identified the most critical behaviors to design for.
After prioritization with Product, Engineering, and the company strategist, the problem decomposed into six discrete challenges:
- Record sharing depends on carrying physical bundles to every appointment
- Storage relies on paper folders that are easily lost or damaged
- Records are written in clinical language patients can't interpret
- Doctors have no snapshot view of the patient's full medical history
- Chronological organization doesn't match how patients recall health events
- No system for medication adherence tracking
Closing the loop
The first design decision was to eliminate manual record entry entirely. Practo Ray, the practice management platform used by 50,000+ doctors, already generated digital prescriptions and records. The infrastructure existed, but the problem was that records stopped flowing once the consultation ended.
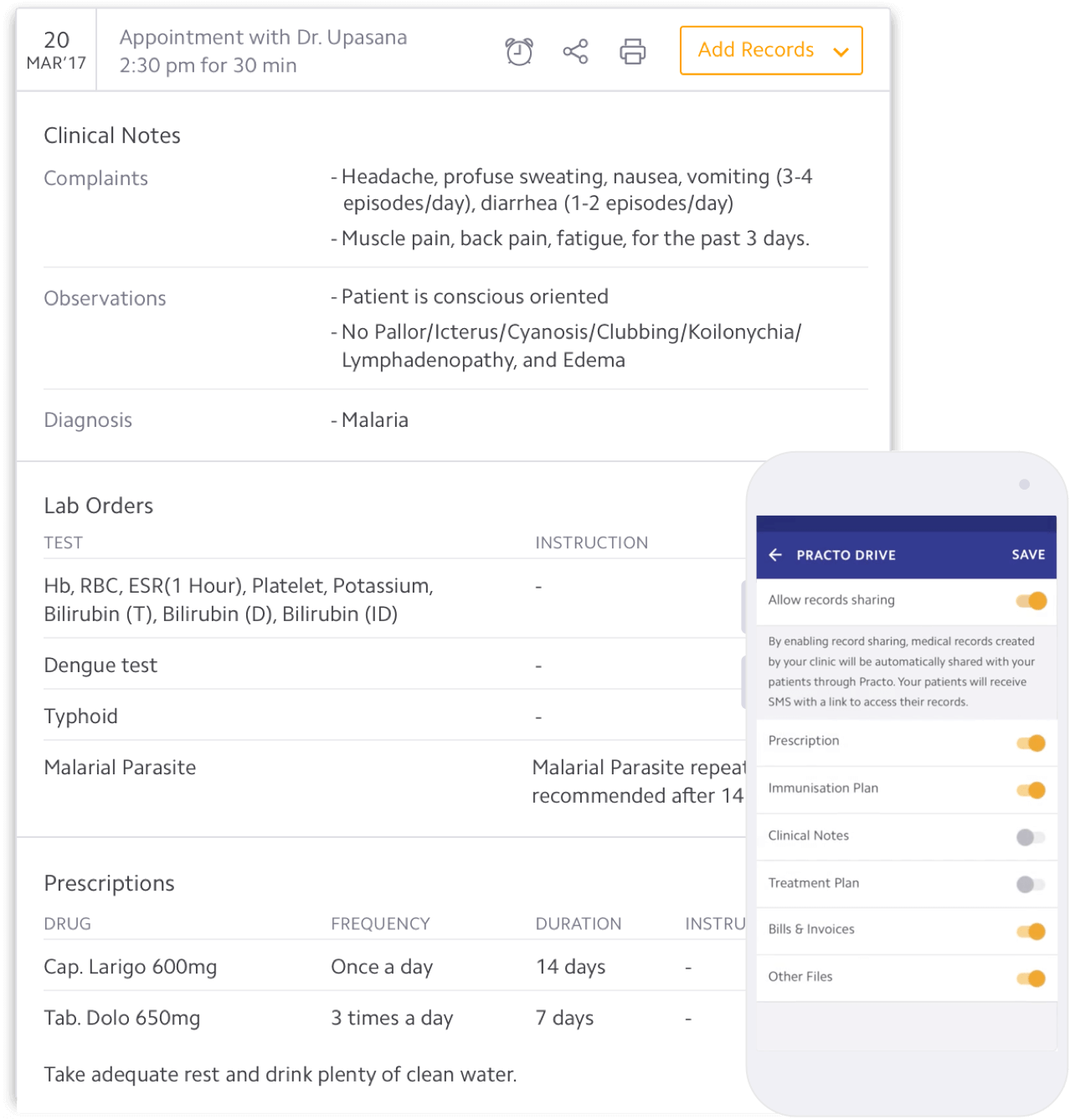
By connecting Ray to the consumer app, every prescription, lab order, and clinical note could flow to the patient automatically. End-to-end encryption ensured privacy. The patient opens their app and their records are already there.
The temporal model
Even with automated record flow, the records themselves were unusable. Research showed that doctors and patients have fundamentally different mental models for health data. Doctors think in systems and diagnoses. Patients think in events and timelines. The patient-facing view needed its own architecture.
After extensive iteration, a temporal model emerged: records structured into upcoming, today, and past, with past items categorized by condition rather than date alone. Secondary research confirmed this approach: doctors increasingly recommend organizing records by problem type, not chronology.
"Any patient's health-history is non-linear. Diseases come and go, against all logical and professional judgment."
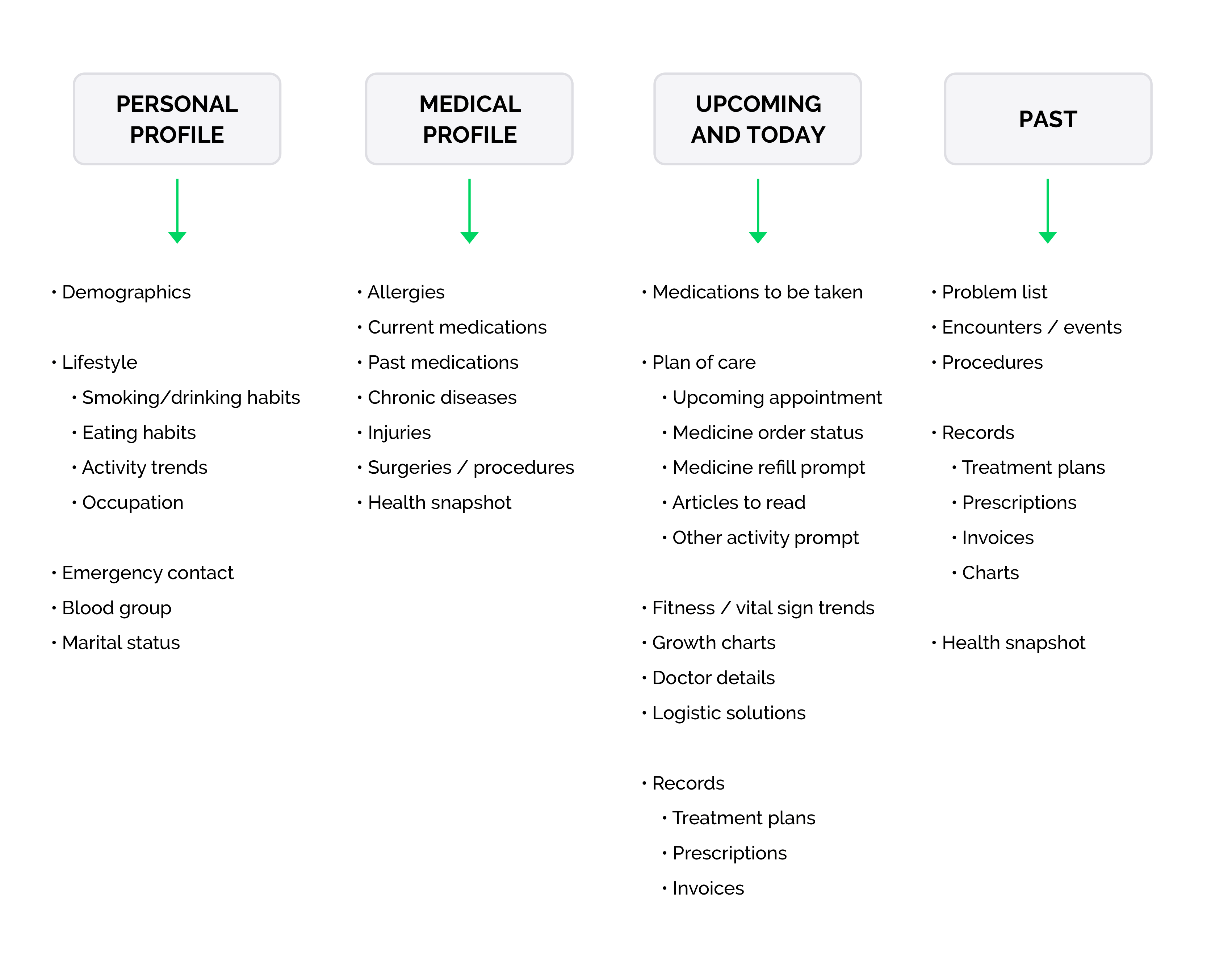
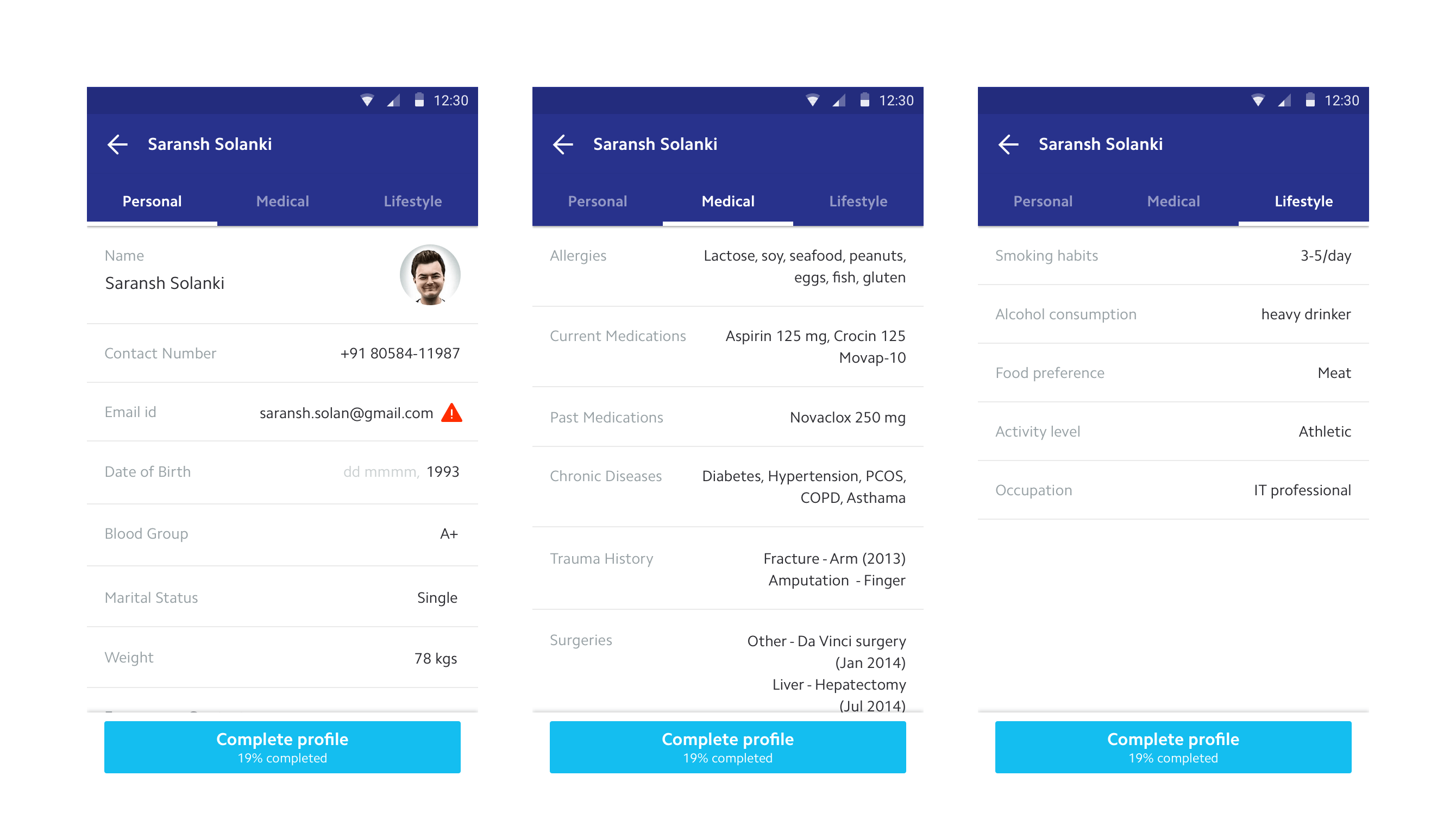
Profile and upcoming
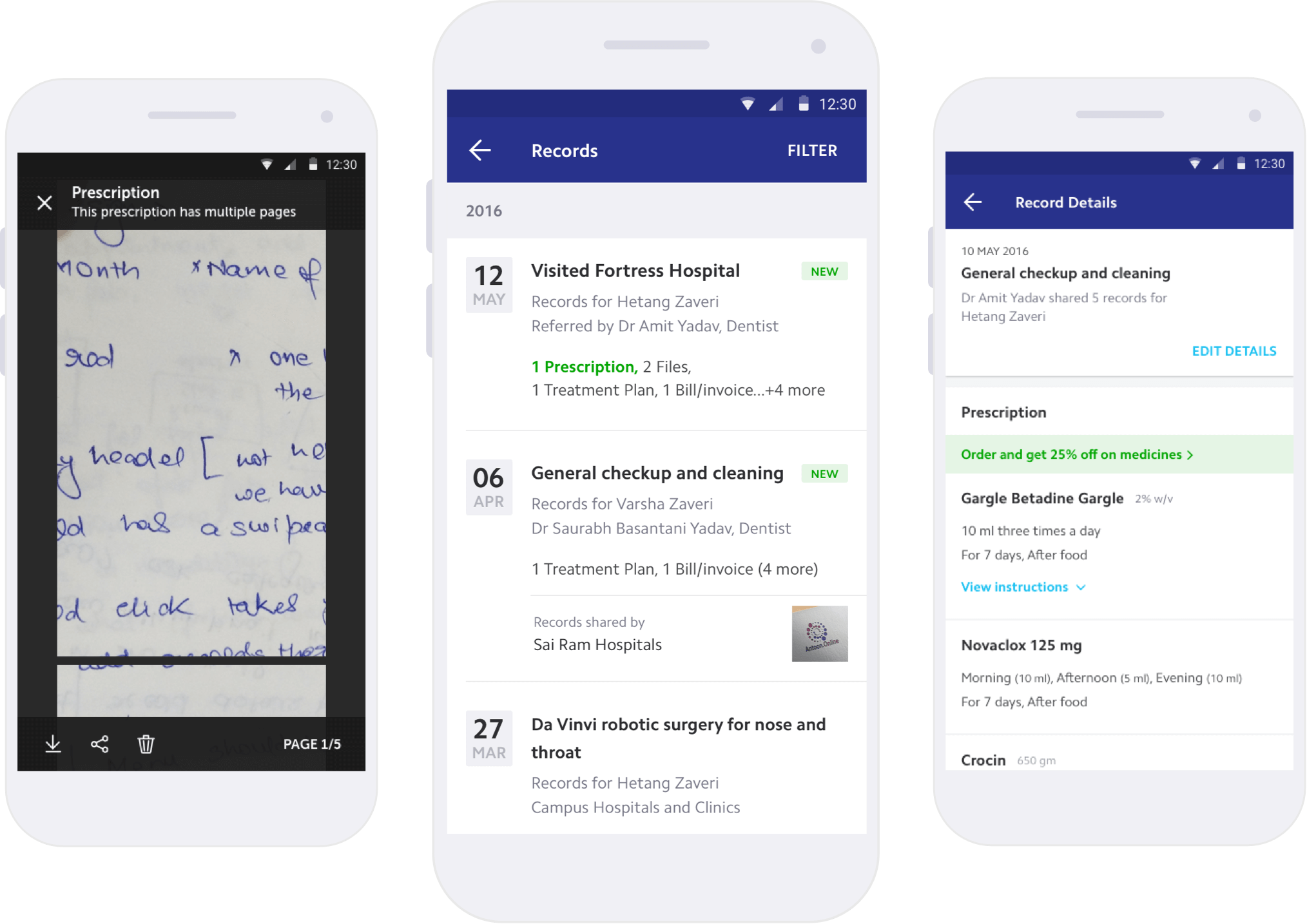
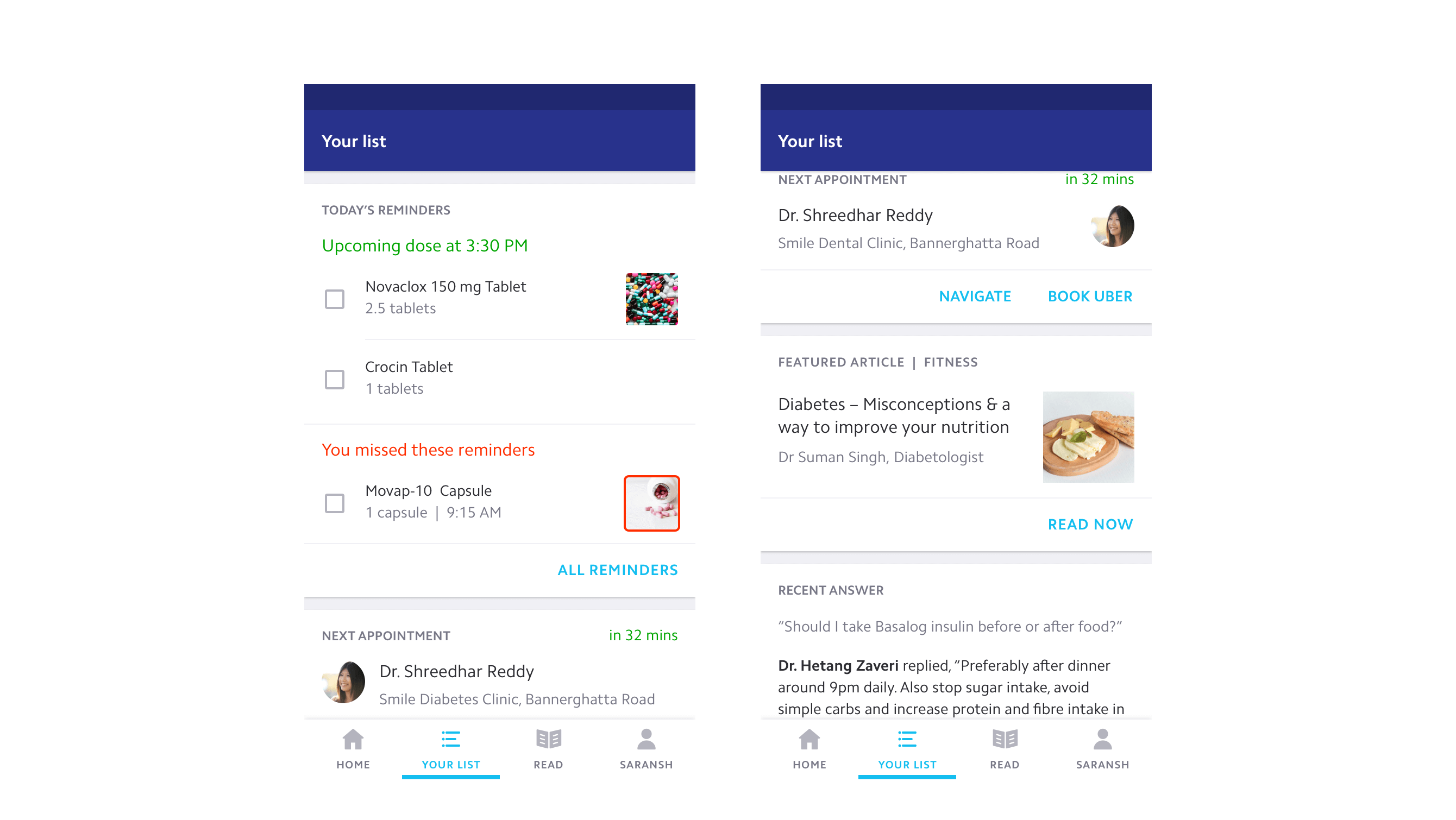
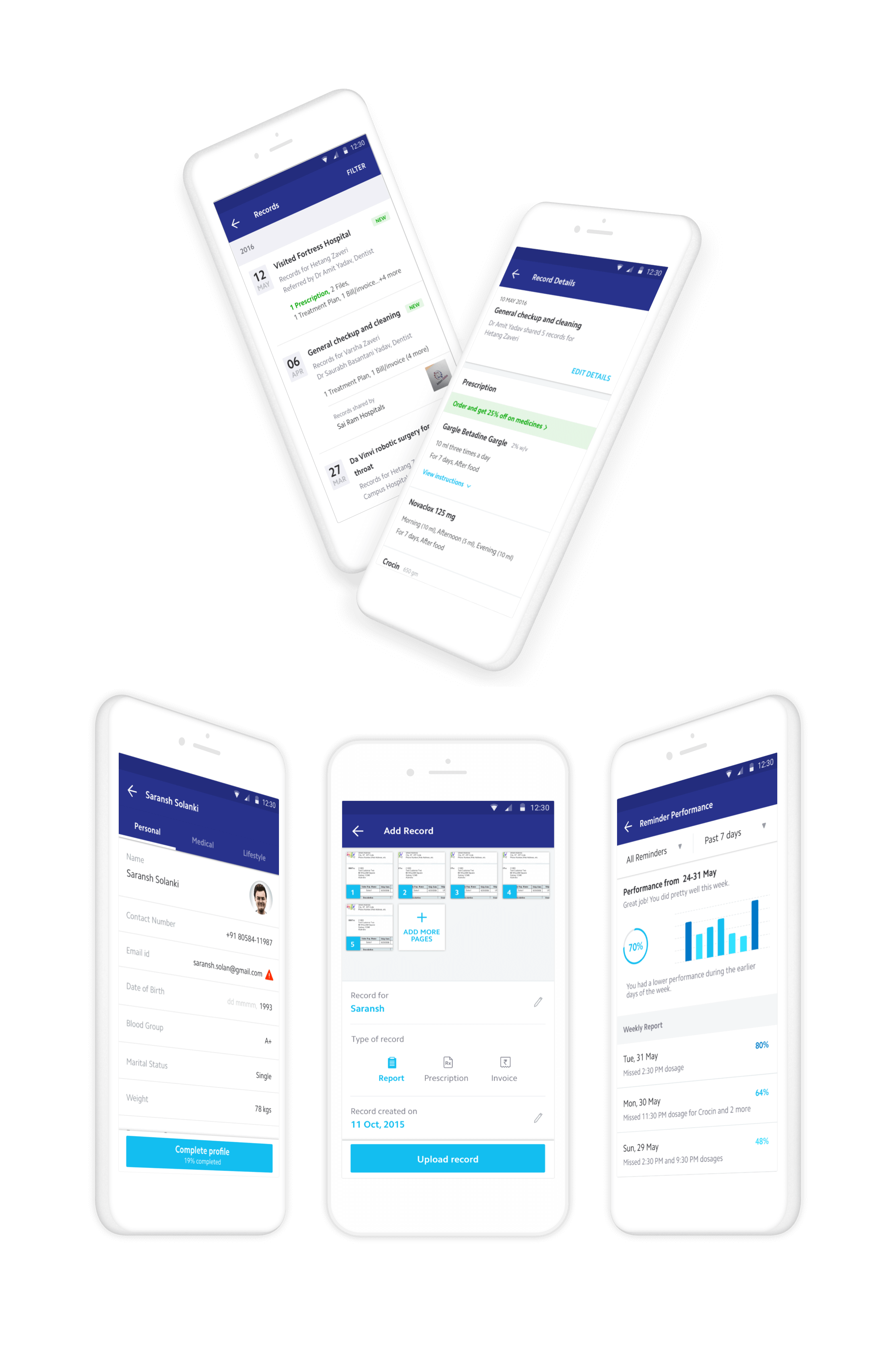
The profile presents patient information in human-readable language rather than a clinical data dump. The upcoming section surfaces only what matters right now (next appointments, pending medications, health insights) displayed in reverse chronological order so the nearest action is always first.
Timeline and history
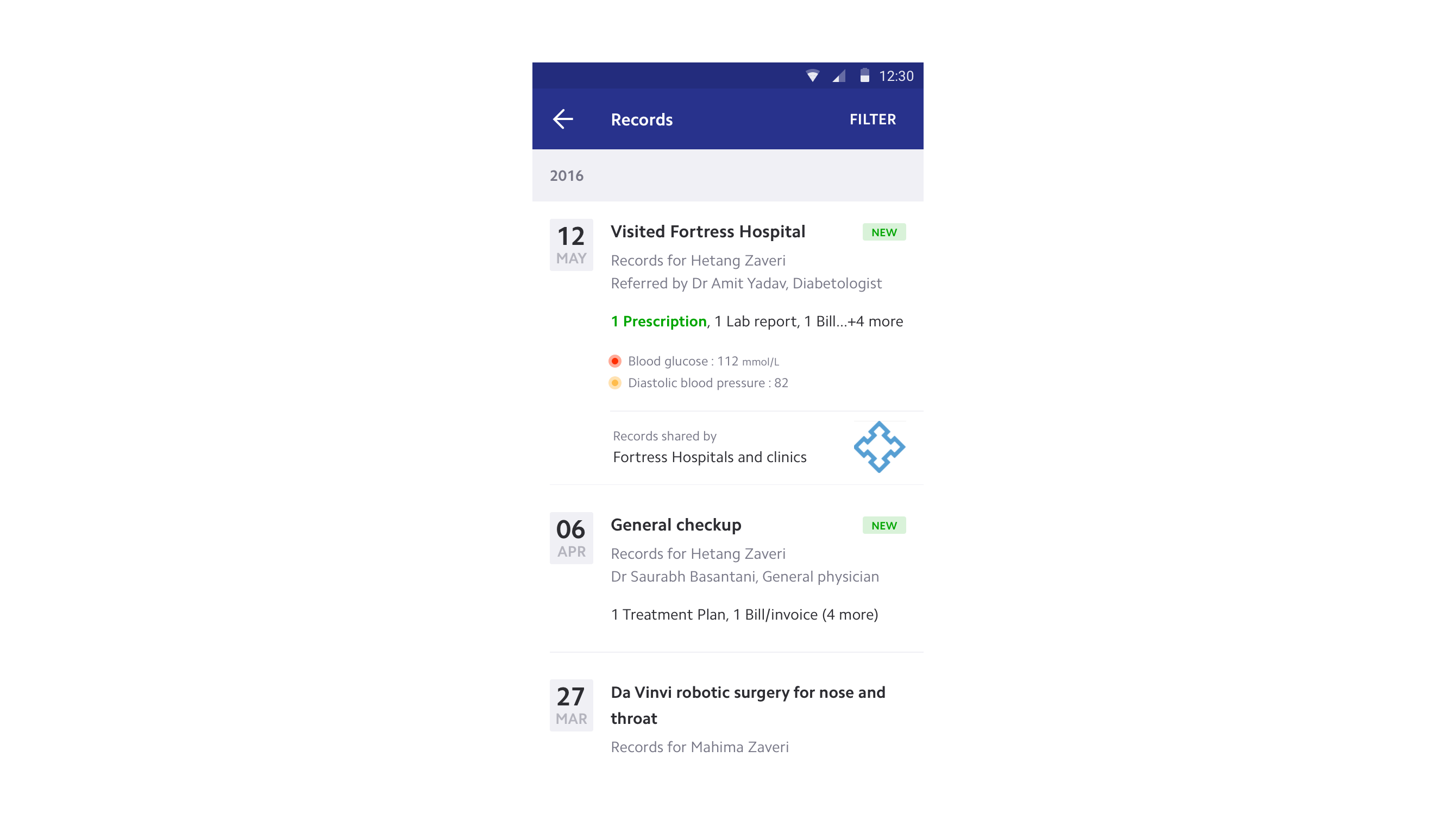
Chronic patients rarely remember medical events by date. They recall the diagnosis, the symptom, the reason they went to the doctor. Each event in the timeline is titled by its purpose, the real story that helps the patient recollect. All prescriptions, records, and medications are linked to their respective events.
For doctors reviewing long-term patients, a snapshot view aggregates providers, visits, medications, and lab results across years. Condition filters let doctors focus on what's relevant to the current consultation.
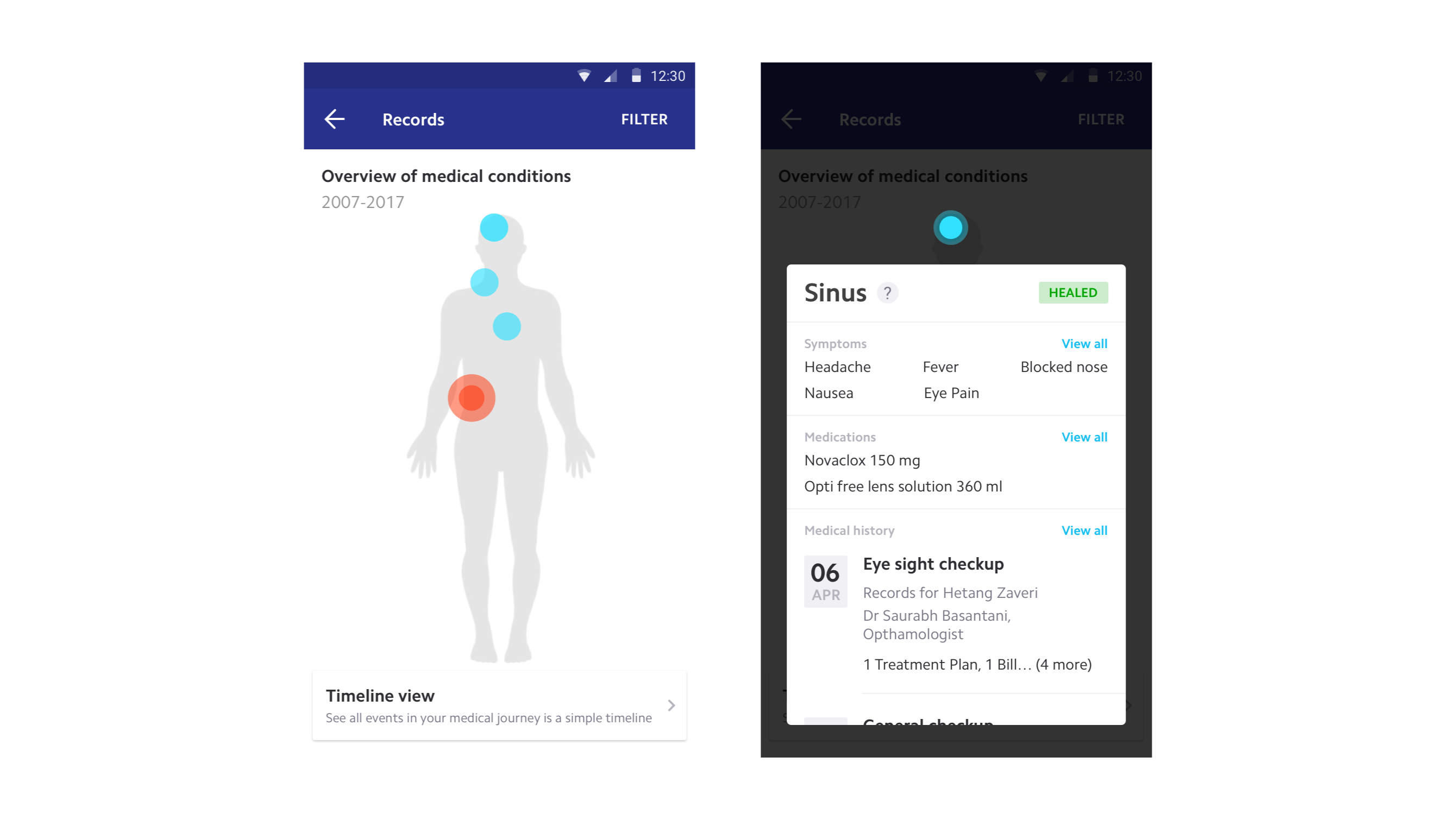
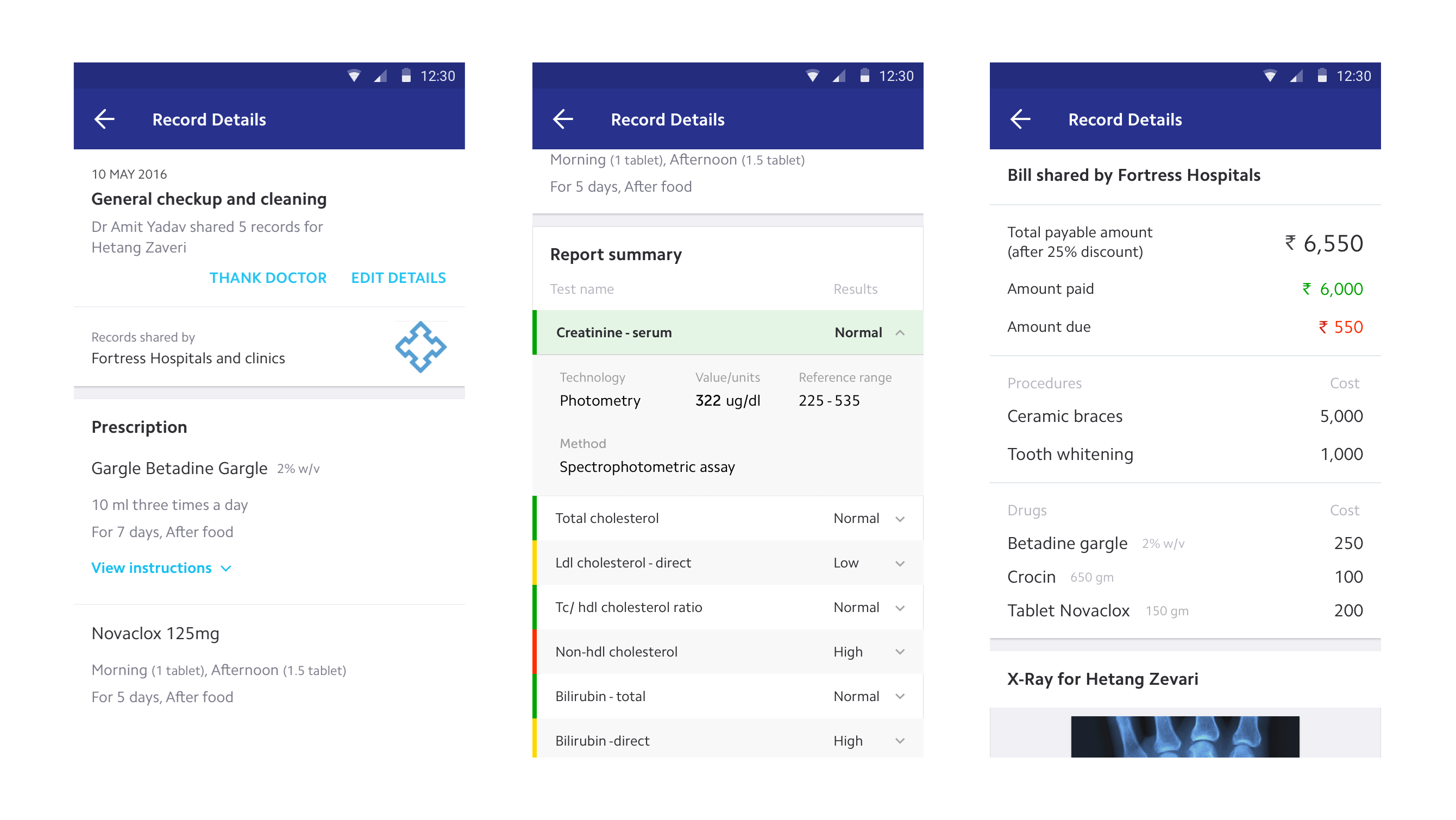
Redesigned records
Each record type was designed independently rather than forced into a single template. Clinical jargon was replaced with natural language. Lab results show whether values are normal or concerning. Prescriptions surface dosage and schedule, not just drug names. The goal: a patient should be able to understand their own medical record without a doctor translating it.
Supporting tools
Not every doctor used Practo Ray, which meant patients still accumulated paper records. A bulk-upload tool enabled patients to photograph and digitize records with metadata in two steps. For medication adherence, I designed a reminder system that became one of Practo's most-used features, detailed in a separate case study.
Medicine reminders ↗What shipped
PHR launched in November 2015 and went through six major updates over the following year. A parallel solution for doctors enabled seamless record sharing from clinic to patient, closing the loop that paper-based systems had left open for decades.
What changed
PHR became foundational to Practo's healthcare strategy. The data flowing through the system enabled better product decisions across the entire platform, from personalized recommendations to adherence insights. The temporal model validated a broader principle: in healthcare, the interface should match the patient's mental model, not the database schema.